
No. 15 | The floor
Coverage loss is the designed federal policy outcome. Here’s what we can still build around it.


In No. 13, I wrote about a number that stayed with me: up to 50% of the 2.8 million Californians in MAGI Medi-Cal expansion could lose coverage not from ineligibility, but from paperwork burden. A paperwork problem. Paperwork problems have solutions.
That argument was right.
The California Budget & Policy Center estimates up to 3.4 million Californians could lose Medi-Cal under H.R. 1. Health Access puts the total at 5 million when federal cuts combine with the state’s own 2025-26 budget. The UC Berkeley Labor Center published county-level projections in March showing where those losses fall. They are not evenly distributed. They fall hardest on the communities Medi-Cal expansion was designed to reach.
This piece asks the question No. 13 didn’t.
After we build the best possible administrative response, after every trusted messenger is deployed and every yellow envelope handled, how many people still lose coverage? Not because the system failed them. Because the policy was designed to remove them.
Coverage loss is the designed federal policy outcome.
Not for everyone. Not even for most people at risk. But for a meaningful portion of the 2.8 million, this is not a documentation failure or a navigation gap. It is what H.R. 1 Section 71119 was written to produce. Naming that clearly is not defeat. It’s what we owe the field.
What MAGI is and why it matters here
Before the Affordable Care Act, Medicaid required a categorical reason to qualify. You had to be elderly, blind, disabled, pregnant, or the parent of a dependent child. Disability required a formal clinical determination.
The Affordable Care Act (ACA) created a new category: Modified Adjusted Gross Income (MAGI) expansion. MAGI Medi-Cal has one test: income. Earn at or below 138% of the federal poverty level, roughly $20,120 per year for an individual in 2026, and you qualify. No disability determination. No asset test. The application became simpler and faster than anything before it.
Millions enrolled who had never had coverage. Among them: millions of people with serious disabilities who chose the MAGI pathway because the old disability process was prohibitively hard and the new one was not. They qualified for disability coverage. They just didn’t go through the disability door.
The 2.8 million adults in California’s MAGI new adult group, aid code M1, ages 19 to 64, have no disability determination on record. The system knows their income. Beginning January 1, 2027, income alone is no longer enough.
MAGI’s simplification was its genius. Under H.R. 1, it became the point of maximum vulnerability.
The four paths
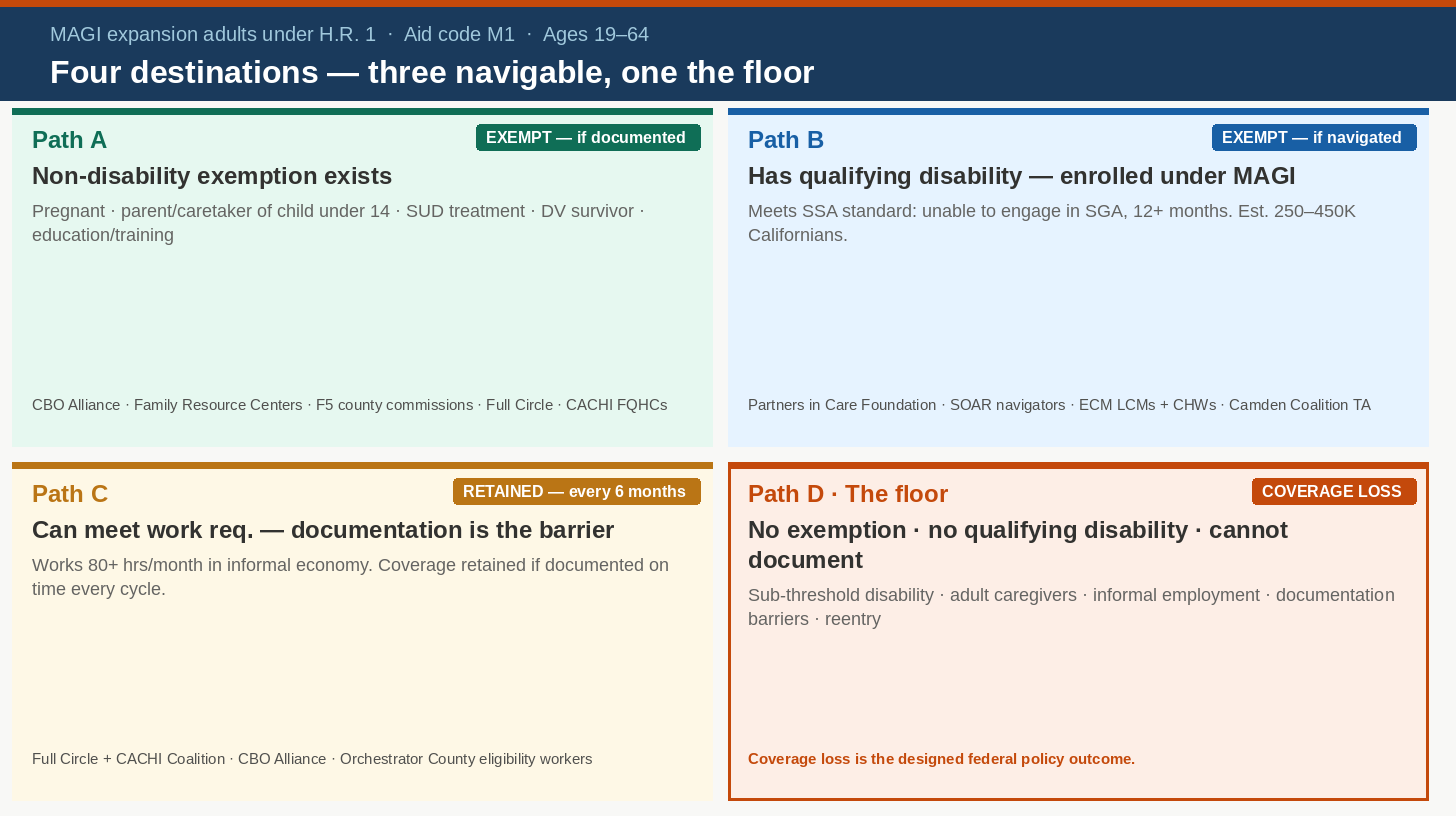
Every MAGI-enrolled Californian facing work requirements will end up in one of four places. Three are navigable. One is the floor.
Path A: has a non-disability exemption, needs documentation
Pregnant women, parents of children under 14, people in substance use treatment, survivors of domestic violence, students in workforce programs. The exemption exists. The coverage is protected, but only if it’s found, recorded, and resubmitted every six months.
Cathryn Couch’s California Community-Based Organization (CBO) Alliance is the right backbone for this work: 700 organizations in all 58 counties, already in members’ lives 40 to 50 times a week. Family Resource Centers hold the direct member relationships. F5 county commissions, funded through Prop 10 in all 58 counties, are the investment and coordination infrastructure that connects resources to delivery organizations. These are distinct kinds of organizations. F5 commissions fund and coordinate; Family Resource Centers deliver. Both are needed. Neither substitutes for the other.
Full Circle Health Network and the California Accountable Communities for Health Initiative (CACHI)-led Medi-Cal Redetermination Coalition are building the documentation workflows and provider training that make Path A survivable at scale.
Path B: has a qualifying disability, enrolled under MAGI, transition possible
With a trained navigator, they could move to an H.R. 1-exempt disability-linked category before enforcement. Partners in Care Foundation, built by June Simmons over decades, shows what fully resourced Supplemental Security Income and Social Security Disability Insurance (SSI/SSDI) navigation looks like: dedicated navigators, legal aid for denials and appeals, health plan integration, a financial model built to last. That model exists. The SOAR (SSI/SSDI Outreach, Access, and Recovery) TA Center that trained navigators nationally closed in August 2025. Path B is a rebuild and replace project. It has to happen before January 2027.
How large is Path B? The disability-qualifying MAGI subset is estimated at 250,000 to 450,000 Californians, a working proxy range because no public figure exists. SOAR-assisted SSI/SSDI approval rates run 65%. Unassisted: 38%. That 27-point gap is the value of what was lost.
Path C: can meet work requirement, documentation is the barrier
The person working 80 hours a month cleaning houses, doing day labor, working gig platforms, whose hours are real but undocumentable to CalHEERS. Or the person who documents one six-month cycle, misses the next, and loses coverage not because they stopped working but because the redetermination clock caught them in a gap.
The Full Circle and CACHI coalition is building the infrastructure for Path C. The binding constraint is the county eligibility worker: the only person who can complete enrollment in CalSAWS. That workforce takes about a year to train fully, turns over at high rates, and now processes redeterminations twice a year. The County Welfare Directors Association estimates California needs more than 2,000 additional eligibility workers to manage the H.R. 1 workload. The Governor’s January 2026 budget proposal does not fund those positions. The administration has indicated the question may be revisited at the May Revision.
Path D: the floor
No exemption applies. The disability is real but doesn’t meet the Social Security Administration (SSA)’s standard: unable to engage in any substantial gainful activity for 12 consecutive months. The work hours are real but undocumentable. The caregiving is genuine but the person being cared for is an adult, and H.R. 1 protects parents of children under 14, not children caring for aging parents.
For Path D, coverage loss is the designed federal policy outcome. Not a documentation failure. The designed outcome.
What a county training deck tells us
In January 2026, a county health system and its managed care partner published a 50-slide redetermination training for providers and community partners. It is well constructed, operationally thorough, and reflects exactly what responsible organizations do in a fast-moving policy environment: they prepared their provider network with the best available guidance.
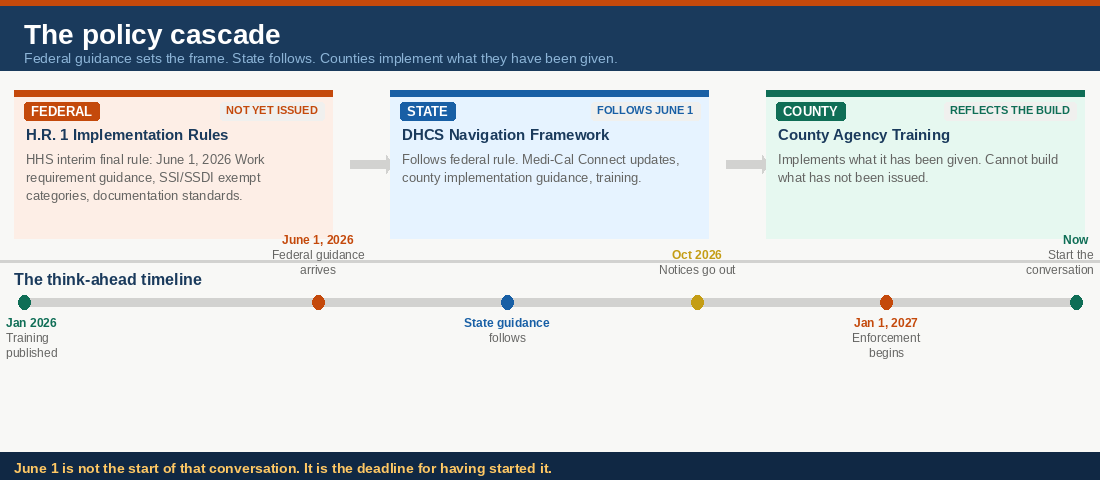
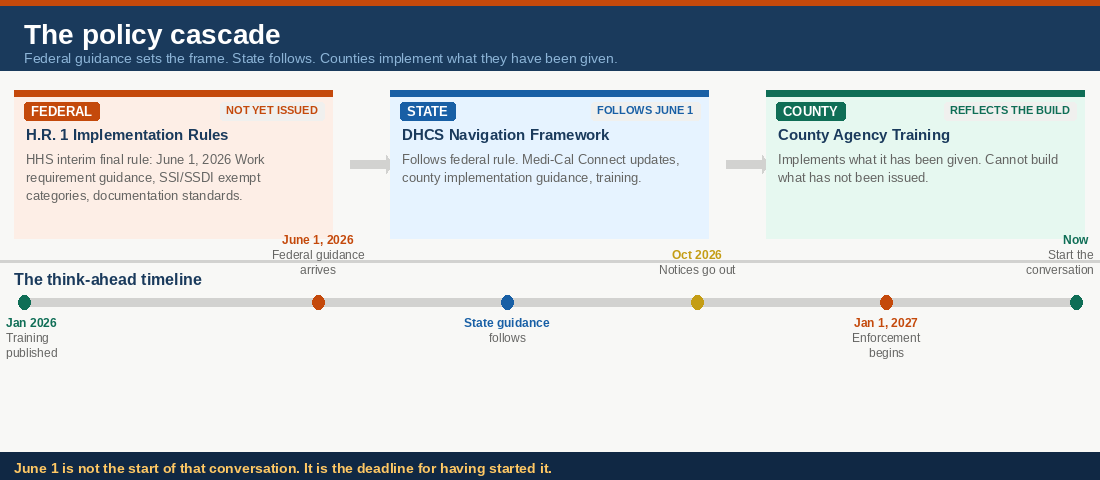
Here is the challenge they were navigating. When that training was published, federal H.R. 1 implementation rules had not been issued. The U.S. Department of Health and Human Services (HHS) interim final rule arrives June 1, 2026, five months after the training was written. The California Department of Health Care Services (DHCS) H.R. 1 Implementation Plan was published January 29, just days before. The Georgetown Center for Children and Families confirmed as of February 1 that the Centers for Medicare & Medicaid Services (CMS) had issued no system modification guidance. The policy framework governing SSI/SSDI transitions had not been written.
You cannot build SSI/SSDI transition guidance into a training when the policy governing those transitions has not been issued. That is not an organizational gap. That is the policy cascade arriving at the delivery level.
Federal guidance comes first. State guidance follows. County agencies implement what they have been given. This training reflects exactly where California is in that sequence: DHCS has built strong MAGI infrastructure. SSI/SSDI transition infrastructure is not yet in the build. That is not a failure of the county. It is the status of the build.
Across all 50 slides: zero mentions of SSI or SSDI pathways. Zero references to the five disability-linked Medi-Cal categories that are H.R. 1 exempt. No guidance on MAGI-to-disability transitions. The disability determination clock is documented at 90 days versus the standard 45-day MAGI clock, correctly documented, without flagging it as a coverage risk. The rules that would define it as one had not been written.
What the training shows is that county infrastructure is MAGI-oriented because Medi-Cal policy has been MAGI-oriented. When federal guidance lands and DHCS issues its navigation framework, the organizations that produced this training will update it. The infrastructure exists. The relationships are in place. The capacity to move is there.
But the counties that respond fastest do not wait for the final guidance packet. They are the ones who started the internal conversation before it arrived. Who asked what their eligibility workers would need to know. Who mapped their CBO navigator capacity before the referral volume came. Who called the table together before the call to action.
June 1 is not the start of that conversation. It is the deadline for having started it.
If you work with or in a county agency, think ahead with them now. Not about what the federal rules will say. We will all read those together in June. About what it would take to be ready when they arrive. Who needs to be in the room before the guidance lands. What your eligibility workers already know about SSI/SSDI pathways. Whether your CBO partners have navigator capacity for Path B members. Whether your provider training can be updated inside 30 days if it needs to be.
The organizations that built that 50-slide training can build the next one. The question is whether the table is set to do it quickly when the time comes.
The gap the training reveals is not organizational failure. The guidance that would close it has not yet been issued.
The choke points nobody is solving
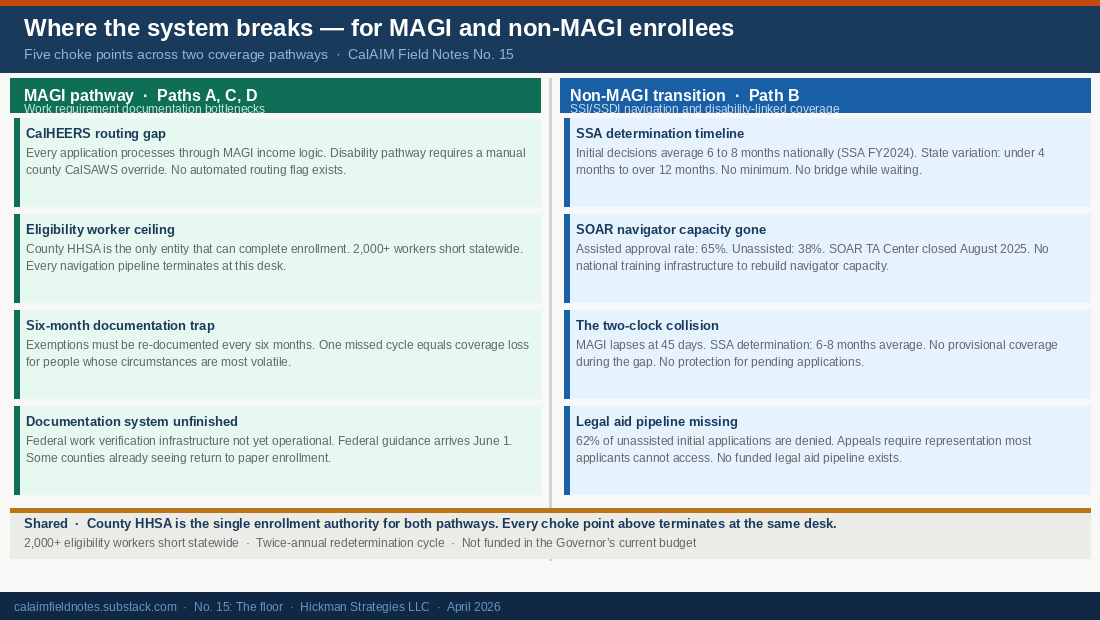
Paths A, B, and C share structural bottlenecks the field is not yet organized around.
The CalHEERS routing gap
Every Medi-Cal application, including from members with serious disabilities, enters CalHEERS first and is processed through MAGI income logic. Getting to a disability pathway requires a county eligibility worker to initiate a manual CalSAWS override. There is no automated disability routing flag. DHCS is rebuilding CalHEERS for H.R. 1 compliance and the build cycle closes January 2027. Adding a routing flag costs less now than after the build closes. Source: Disability Rights California and CalHEERS RFI No. 73050004 (May 2024).
The eligibility worker ceiling
The county Health and Human Services Agency (HHSA) is the only entity legally able to complete enrollment in CalSAWS. CBOs, federally qualified health centers (FQHCs), Family Resource Centers, F5 county commissions, and Enhanced Care Management (ECM) partners can assist, counsel, and prepare. They cannot enroll. Every navigation pipeline terminates at a county eligibility worker desk, a desk that is already 2,000 workers short statewide.
The six-month documentation trap
Path A exemptions are not a one-time protection. They must be re-documented every six months. One missed cycle equals coverage loss. For people whose circumstances are volatile, moving, changing providers, leaving a shelter, the cycle is not a procedure. It is a trap.
The documentation system is not finished
Federal implementation guidance arrives June 1, 2026, seven months before enforcement. The work verification infrastructure is not yet operational. Some counties are already seeing MAGI members return to paper-based enrollment, a signal that digital-first assumptions in the build are running ahead of the actual population.
The four bottlenecks above run across all MAGI paths. Path B carries two more that are its own.
The two-clock collision
The MAGI redetermination clock runs 45 days. SSA initial disability determinations average 6 to 8 months nationally, and longer in high-volume states. There is no bridge coverage for the gap between them. A Path B member who loses MAGI coverage while their disability application is still pending has no coverage until the determination lands. No provisional protection exists for applications in process. The two clocks do not connect.
The legal aid pipeline
Sixty-two percent of unassisted SSI/SSDI initial applications are denied. An appeal requires legal representation. Most applicants cannot access it. California has no funded legal aid pipeline connected to the CalHEERS or CalSAWS ecosystem. SOAR-trained navigators were the closest thing to that infrastructure. The SOAR TA Center closed in August 2025. What remains is a 62% denial rate and no systematic path to contest it.
Who is in Path D
The sub-threshold disability: fibromyalgia, episodic depression, long COVID, chronic pain that impairs work on some days and not others. Real limitation. Doesn’t meet the SSA’s 12-month durability standard. The condition is disabling. It doesn’t qualify.
The adult caregiver: the daughter who left work to care for her mother with advancing dementia. H.R. 1 protects parents of children under 14. It does not protect adult children caring for aging parents, spouses caring for disabled partners, or siblings caring for siblings. Caregiving of adults is not a qualifying work activity. It is invisible to the statute.
The informal worker: cleaning houses, picking crops, doing day labor. Working, often exhaustingly, in the cash economy. The hours are real. CalHEERS cannot verify them. Coverage loss comes not from failure to work but from inability to document work in a form the system accepts.
The person cycling through employment: seasonal, part-time, interrupted by illness or caregiving. Works enough months to qualify. Misses one six-month window. Loses coverage. Re-enrolls. Misses the next one.
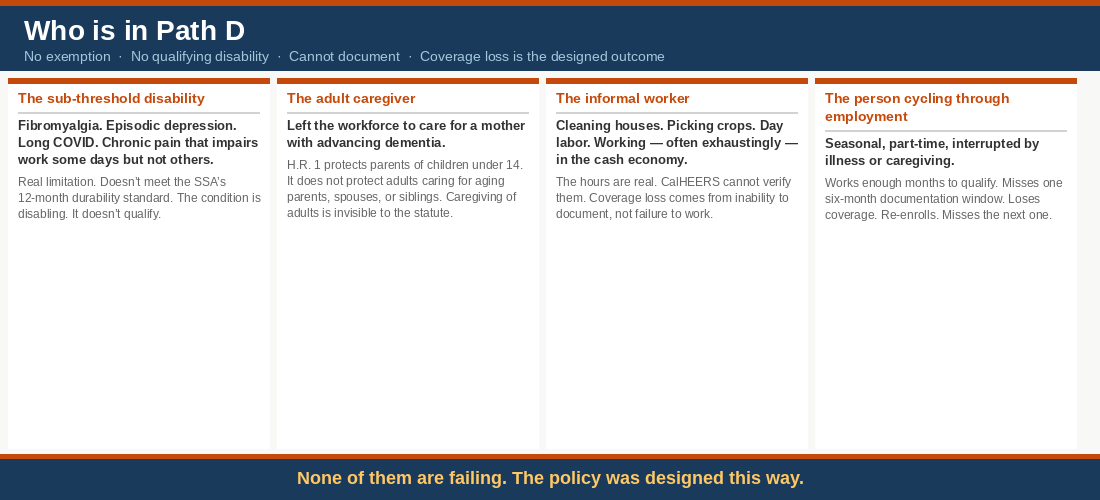
None of them are failing. The policy was designed this way.
San Diego and Imperial Counties: Path D made real
The clearest example of what Path D looks like is already unfolding.
A March 4, 2026 briefing circulated among health system partners in San Diego and Imperial Counties named the plain reality: when people lose Medi-Cal and have nowhere else to go, they end up in the hospital. Neither San Diego nor Imperial County has a county hospital.
California Welfare and Institutions Code Section 17000 establishes that counties must serve as the provider of last resort for residents who do not qualify for Medi-Cal. The County Medical Services Program in Imperial County and County Medical Services in San Diego are the legal infrastructure for that obligation. Both have been largely unfunded for years. CMS currently has three people enrolled.
The San Diego County Board of Supervisors voted 4-1 in early March to begin overhauling CMS, directing a comprehensive review through its Ad Hoc Subcommittee on Social Safety Net and Behavioral Health Systems Transformation. One hundred and fifty thousand San Diegans have already left the Medi-Cal rolls in recent years without leaving San Diego. H.R. 1 coverage losses arrive on top of that.
From the March 4, 2026 briefing:
“You know all too well that when an uninsured person needs care, it’s your hospitals where they end up.”
This is not a planning scenario. This is Path D arriving early in a region that is watching it come.
The Orchestrator County
The counties that respond best to H.R. 1 will not be the ones that process redeterminations most efficiently. They will be the ones that coordinate the full ecosystem: the CBO Alliance, Family Resource Centers, F5 county commissions, FQHCs, health plans, ECM providers, and the navigator organizations working Path B, into a single legible response system with the county at the center.
The Orchestrator County model rests on one structural fact: county government is the only entity that can complete enrollment in CalSAWS. Everything else flows from that. Counties that exercise that authority actively multiply the impact of every organization they coordinate. That means convening the full provider network, integrating F5 commissions and Family Resource Centers into outreach workflows, coordinating Path B referral pipelines with ECM providers, and making the board-level case for eligibility worker investment before the coverage losses materialize, not in response to them.
The San Diego Board response is a model: a board-level commitment, an ad hoc subcommittee, an explicit accountability structure, and an honest acknowledgment that the legal obligation has been structurally unfunded for years and is about to matter enormously.
What we can still build
The possibilist’s argument is not that everything is possible. It is that the possible is larger than we are currently building toward, and that naming the limits honestly is how we stay inside them.
For Paths A, B, and C, perhaps 800,000 to 1.2 million people, the window is open. CBO Alliance coordination needs to be funded before October 2026 notices go out, not in response to January 2027 coverage losses. A CalHEERS disability routing flag added during the current build cycle would multiply every navigator in the system. County eligibility worker capacity needs board-level budget protection now. ECM providers need to build Path B navigator capacity as a funded function, not absorb it informally into unreimbursed community supports.
For Path D: document who lands there. Track what happens, the deferred care, the emergency visits, the Section 17000 programs being rebuilt from three enrolled members. Build the evidence base that makes the policy argument to Sacramento and to Congress. Make sure the safety net knows Path D is coming.
The floor is not the ceiling. The floor is where we start building.
What’s the first specific, measurable commitment?
In No. 13, the organizing question was: do we have a specific, measurable plan to close our share of the administrative gap before Q3?
This piece adds a second: do we have a specific, measurable plan to track what happens to the people the administrative response cannot reach?
Both questions need answers before October. Because the people in Path D, the people the policy was designed to leave behind, deserve to be counted. Counting is how we prove, a year from now, that this policy had a floor, and that we saw it, and that we said so.
The work that begins January 2, 2027 has to be organized before January 1.
Coverage loss is the designed outcome. What gets built from this floor is ours to design.
* The 250,000-450,000 disability-qualifying MAGI subset is a working proxy estimate. No public figure exists. DHCS claims data analysis would establish a citable number. The 1.4 million paperwork-failure figure is DHCS’s own projection from the February 5, 2026 webinar.
Sources
– DHCS H.R. 1 Implementation Plan Overview Webinar, February 5, 2026.
– H.R. 1 §71119 (One Big Beautiful Bill Act), signed July 2025.
– California Budget & Policy Center (2025): up to 3.4 million Californians could lose Medi-Cal.
– Health Access, “The State of Health Care Coverage” (2025): up to 5 million losing coverage.
– UC Berkeley Labor Center, county-level projections (March 2026).
– County Welfare Directors Association of California (Chico News & Review, March 23, 2026): 2,000+ additional eligibility workers needed; not funded in Governor’s proposed budget.
– County-level provider redetermination training (January 2026). Reviewed through provider network channels. Source protected.
– Homeless Leadership Coalition / SOAR TA Center closure, August 18, 2025.
– SSA FY2024 Agency Financial Report: 1.18 million initial claims pending nationally.
– SSA FY2024 Workload Data: 38% initial approval rate; 65% SOAR-assisted.
– SSA OIG Audit, July 2025: 222-day California initial decision average.
– Disability Rights California; CalHEERS RFI No. 73050004, May 2024.
– DHCS HR-1 Implementation Plan, January 29, 2026.
– San Diego / Imperial Counties biweekly briefing, March 4, 2026.
– California Welfare and Institutions Code §17000.
– LAO, “Considering Medi-Cal in the Midst of a Changing Fiscal and Policy Landscape,” October 2025.